


Background: We recently reported on the single-institution experience with allogeneic hematopoietic stem cell transplantation (HSCT) in 22 consecutive patients with GATA2 deficiency or the MonoMAC syndrome and observed a disease-free survival of nearly 90%. However, despite 10/10 HLA match of matched related donors (MRD) and matched unrelated donors (URD), there was a 25% incidence of grades III-IV acute graft-versus-host disease (GVHD) with tacrolimus/methotrexate (Tacro/MTX). In contrast, there was no grade III-IV acute GVHD in the haploidentical related donor (HRD) recipients, all of whom received GVHD prophylaxis with post-transplantation cyclophosphamide (PT/Cy) followed by tacrolimus/mycophenolate (tacro/MMF). Based on this initial experience, the protocol was subsequently amended to incorporate PT/Cy in all patients. We now report on this expanded cohort of a total of 59 patients, representing the largest experience with HSCT for GATA2 deficiency.
Methods: This single-institution study was conducted at the National Institutes of Health Clinical Center between 2013 and 2020 (ClinicalTrials.gov Identifier: NCT01861106). Patients between 12 to 60 years of age were eligible if they had a deleterious mutation in the GATA2 gene, or clinical picture of the MonoMAC syndrome. Although the primary endpoints were engraftment and reversal of the clinical phenotype, a secondary endpoint was added to determine if PT/Cy in the MRD and URD reduced the incidence of grade III-IV aGVHD without compromising the overall and disease-free survival. Immune reconstitution at 100 days, 6, 12, 24, 36 months was analyzed.
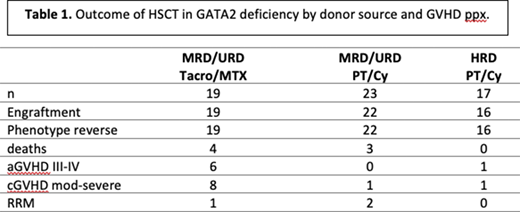
Results: 59 patients (median age at diagnosis 24 years; IQR 20-32) with GATA2 deficiency or the MonoMAC syndrome underwent allogeneic HSCT. MRD and URD recipients received busulfan for four days (targeted to an AUC 3600-4800) and fludarabine, whereas HRD recipients received two days of low dose cyclophosphamide, 5 days fludarabine, 200cGY total body irradiation, and two or three days of busulfan depending upon the presence or absence of clonal cytogenetic abnormalities. Donor sources included: 11 MRD, 31 URD, and 17 HRD. Median follow-up was 2 years [IQR 1-4], 88% (52/59) are currently alive. Seven deaths have occurred, including: persistent AML (n=1); infection (n=4); poor graft function and cardiac arrest (n=1) and from HPV-associated metastatic cancer (n=1). All of the patients who received HRD transplant are alive. Median time to neutrophil engraftment was 15 days (IQR 13-17) and 19.5 days (IQR 16-25) for platelets. Ninety three percent (55/59) of patients had blood test results after 100 days post-transplant to assess immune reconstitution; eighty one percent (45/55) had normal absolute monocyte counts, 67% (37/55) had normal absolute NK cell counts and 89% (49/55) had normal B cells counts. There was one case of primary graft failure in a recipient of an URD-transplant, and one secondary graft rejection in a recipient of HRD-transplant. Fifty-four percent (32/59) of patients had pre-HSCT myelodysplastic syndrome (MDS), and only two relapsed post-HSCT. Forty two percent (25/59) had abnormal cytogenetics pre-HSCT; amongst 23 patients with serial pre/post bone marrow cytogenetic evaluations, 19 had established normal cytogenetics post-HSCT. Forty five percent (19/42) of MRD/URD patients received Tacro/MTX for GVHD prophylaxis, and 31.5% (6/19) developed grade III-IV acute GVHD (aGVHD). In contrast, 55% (23/42) MRD/URD patients received PT/Cy for GVHD prophylaxis, and none developed grade III-IV aGVHD (p 0.0052). Five percent (1/17) of HRD recipients developed grade III-IV aGVHD. Forty two percent (8/19) of MRD/URD patients who received post-transplant Tacro/MTX had chronic GVHD, 4.3% (1/23) of MRD/URD patients who received PT/Cy developed cGVHD, and 5.8% (1/17) of HRD patients developed cGVHD within the first 2 years post-transplant.
Conclusions: Allogeneic HSCT using a busulfan-based regimen in GATA2 deficiency results in nearly a 90% disease-free survival with long-term immune reconstitution. The use of PT-Cy reduced the risk of severe aGVHD and cGVHD and did not increase the risk of relapse or progression of MDS/AML. With earlier recognition of the disease, and the use of PT/Cy more broadly, these results are expected to continue to improve.
Notarangelo:NIAID, NIH: Research Funding.
This icon denotes a clinically relevant abstract

